
First published 2019
From the day of diagnosis, I spent the 2 weeks totally non weight bearing, unable to get upstairs or do anything for myself, and my daughters Emma and Sarah and carer Georgie looked after me with dedication above and beyond the call of duty.
They did all my food preparation household chores and assisted with personal hygiene and even managed the procurement of appliances to help with the non-weight bearing regime, I.e. stairlift, scooter, wheelchair, commode and knee on stroller etc.
Thanks to the early diagnosis by my Podiatrist Colin, and his tenacity to get me seen urgently by Dr Khaleel’s team and with help from Dr. Khaleel’s Team the condition is now under control, and for that, I am extremely grateful.
I was initially attending the Rowley Bristow treatment centre three times a week and was expertly treated by the two Helen’s, Kelly, Nikki, Tracy and Gemma. I am currently attending once a week and hope to be fitted for a surgical boot soon.


I would also like to thank all my friends
who have given me moral support during my struggle with charots foot
Andi, Jules, Nick,
Dave, Brian, Peter,
Tony, Rob, Les,
Pat, Gary, Steve
…to name just a few!
Early diagnosis and treatment can prevent more damage and avoid deformity and other complications.
Treatment has three goals: take the weight off the foot, treat bone disease (usually with cast; bisphosphonates and other supplements are sometimes used) and prevent new foot fractures.
Nonsurgical treatment for Charcot foot consists of: Immobilization.
Because the foot and ankle are so fragile during the early stage of Charcot, they must be protected so the weakened bones can repair themselves.
It may take the bones several months to heal, although it can take considerably longer in some patients.
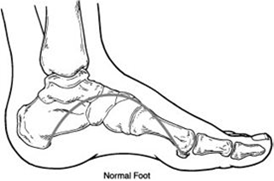
Charcot Foot
What Is Charcot Foot?
Charcot foot is a condition causing weakening of the bones in the foot that can occur in people who have significant nerve damage (neuropathy).
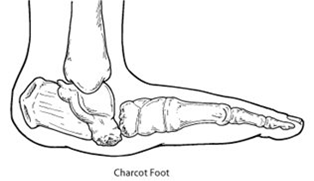
The bones are weakened enough to fracture, and with continued walking, the foot eventually changes shape.
As the disorder progresses, the joints collapse and the foot takes on an abnormal shape, such as a rocker-bottom appearance.
Charcot foot is a serious condition that can lead to severe deformity, disability and even amputation.
Because of its seriousness, it is important that patients living with diabetes—a disease often associated with neuropathy—take preventive measures and seek immediate care if signs or symptoms appear.
Causes
Charcot foot develops as a result of neuropathy, which decreases sensation and the ability to feel temperature, pain or trauma.
Because of diminished sensation, the patient may continue to walk—making the injury worse.
People with neuropathy (especially those who have had it for a long time) are at risk for developing Charcot foot.
In addition, neuropathic patients with a tight Achilles tendon have been shown to have a tendency to develop Charcot foot.
Symptoms
The symptoms of Charcot foot may include:
- Warmth to the touch (the affected foot feels warmer than the other)
- Redness in the foot
- Swelling in the area
- Pain or soreness
Diagnosis
Early diagnosis of Charcot foot is extremely important for successful treatment.
To arrive at a diagnosis, the surgeon will examine the foot and ankle and ask about events that may have occurred prior to the symptoms.
X-rays and other imaging studies and tests may be ordered.
Once treatment begins, x-rays are taken periodically to aid in evaluating the status of the condition.
Nonsurgical Treatment
It is extremely important to follow the surgeon’s treatment plan for Charcot foot.
Failure to do so can lead to the loss of a toe, foot, leg or life.
Nonsurgical treatment for Charcot foot consists of:
Immobilization.
- Because the foot and ankle are so fragile during the early stage of Charcot, they must be protected so the weakened bones can repair themselves. Complete no weight-bearing is necessary to keep the foot from further collapsing.
- The patient will not be able to walk on the affected foot until the surgeon determines it is safe to do so.
- During this period, the patient may be fitted with a cast, removable boot or brace and may be required to use crutches or a wheelchair.
- It may take the bones several months to heal, although it can take considerably longer in some patients.
Custom shoes and bracing.
- Shoes with special inserts may be needed after the bones have healed to enable the patient to return to daily activities—as well as help prevent recurrence of Charcot foot, development of ulcers and possibly amputation. In cases with significant deformity, bracing is also required.
Activity modification.
- A modification in activity level may be needed to avoid repetitive trauma to both feet.
- A patient with Charcot in one foot is more likely to develop it in the other foot, so measures must be taken to protect both feet.
When Is Surgery Needed?
In some cases, the Charcot deformity may become severe enough that surgery is necessary.
The foot and ankle surgeon will determine the proper timing as well as the appropriate procedure for the individual case.
Preventive Care
The patient can play a vital role in preventing Charcot foot and its complications by following these measures:
- Keeping blood sugar levels under control can help reduce the progression of nerve damage in the feet.
- Get regular check-ups from a foot and ankle surgeon.
- Check both feet every day—and see a surgeon immediately if you notice signs of Charcot foot.
- Be careful to avoid injury, such as bumping the foot or overdoing an exercise program.
- Follow the surgeon’s instructions for long-term treatment to prevent recurrences, ulcers and amputation.
- Charcot foot can make walking difficult or impossible, and in severe cases can require amputation.
- But a surgical technique that secures foot bones with an external frame has enabled more than 90 percent of patients to walk normally again, according to Loyola University Health System foot and ankle surgeon Dr.16 Jul 2010
- The alarming increase of morbidly obese diabetics is causing more new cases of a debilitating foot deformity called Charcot foot.
- Charcot foot can make walking difficult or impossible, and in severe cases can require amputation.
- But a surgical technique that secures foot bones with an external frame has enabled more than 90 percent of patients to walk normally again, according to Loyola University Health System foot and ankle surgeon Dr. Michael Pinzur. Pinzur, one of the nation’s leading surgeons who treat Charcot foot, describes the device in the journal Hospital Practice.
- The device, called a circular external fixator, is a rigid frame made of stainless steel and aircraft-grade aluminium.
- It contains three rings that surround the foot and lower calf.
- The rings have stainless-steel pins that extend to the foot and secure the bones after surgery.
- The fixator “has been demonstrated to achieve a high potential for enhanced clinical outcomes with a minimal risk for treatment-associated morbidity,” Pinzer wrote. Pinzur treats about 75 Charcot patients per year with external fixators.
- Most of these patients are diabetics.
- Charcot foot can occur in a diabetic who has neuropathy (nerve damage) in the foot that impairs the ability to feel pain.
- Charot foot typically occurs following a minor injury, such as a sprain or stress fracture.
- Because the patient doesn’t feel the injury, he or she continues to walk, making the injury worse. Bones fracture, joints
- collapse and the foot becomes deformed.
- The patient walks on the side of the foot and develops pressure sores.
- Bones can become infected.
- The obesity epidemic is increasing the incidence of Charcot foot in two ways.
- The excess weight increases the risk of diabetic neuropathy, as well as the risk that patients with diabetic neuropathy will develop Charcot foot.
- There has been an alarming increase in morbid obesity among diabetics.
- About 62 percent of U.S. adults with Type 2 diabetes now are obese, and 21 percent are morbidly obese, according to a 2009 study by Loyola kidney specialist Dr. Holly Kramer and colleagues published in the Journal of Diabetes and its Complications.
- Morbid obesity is defined as having a body mass index (BMI) greater than 40.
- For example, a person who is 5-foot, 10-inches tall and has a BMI of 40 weighs 278 pounds.
- Traditional surgical techniques, in which bones are held in place by internal plates and screws, don’t work with a subset of obese Charcot patients.
- Their bones, already weakened by complications of Charcot foot, could collapse under the patient’s heavy weight.
- A common treatment in such cases is to put the patient in a cast.
- But bones can heal in deformed positions.
- And it is difficult or impossible for obese patients to walk on one leg when the other leg is in a cast.
- Patients typically must use wheelchairs and are confined to the first story of the house for as long as nine months.
- And after the cast comes off, they must wear a cumbersome leg brace.
- By contrast, patients who are treated with an external fixator often can walk or at least bear some weight on the treated leg.
- The device is attached to the leg for only two or three months.
- A 2007 study by Pinzer, published in Foot & Ankle International, demonstrated the benefits of the external fixator.
- Pinzur followed 26 obese, diabetic Charcot foot patients who had an average body mass index of 38.3.
- After surgery to correct the deformity, the foot bones were held in place by the external fixator.
- A year or more later, 24 of the 26 patients (92 percent) had no ulcers or bone infections and were able to walk without braces, wearing commercially available shoes designed for diabetics.